One of Santa’s myriad helpers recently handed me an Auvon AS8016 TENS/EMS Unit. The manual is, shall we say, light on tech details, but some casual searching turns up the general specs for medical-grade units found in physical therapy offices, plus adjacent Rule 34 compliant (i.e. NSFW) offerings.
Being that type of guy, I had to look at the electricity. Somewhat to my surprise, the reference load turns out to be a pure 500 Ω resistance, which is easy enough to cobble up from a pair of 1 kΩ resistors:
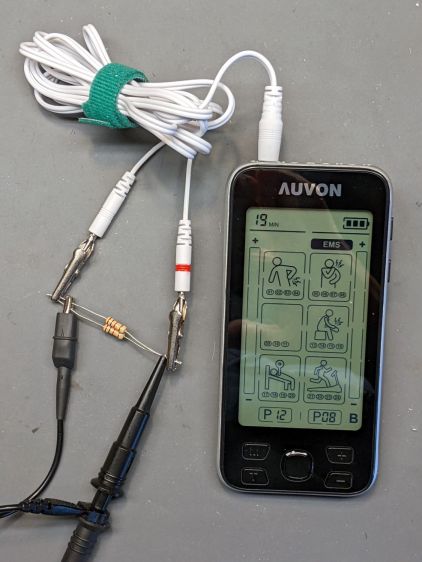
The alligator clips crunched around the 2 mm pins are not appropriate for even a brutal e-stim session; they’re from the Small Drawer of Test Connectors, to which they shall return unblooded.
The red Sharpie highlight around one pin identifies the center conductor of the two-wire cable, as determined by simple continuity testing:

The 22 mil = 0.5 mm wire (from the Little Tin o’ Snippets) fits snugly into the coaxial connector’s center contact; one could probably slip a rounded shim between the shell and the outer contact, perhaps to debug an intermittent connection. Note that the connectors on both ends of the wires are not standardized among various TENS/EMS manufacturers.
The AS8016 has two pairs of connectors:

The A1 and A2 jacks are wired in parallel, as are the B1 and B2 jacks, with the A pair galvanically isolated from the B pair. You can set the modes / programs / pulse parameters differently for A and B. Although the manual doesn’t mention it, using the A and B channels (perhaps with the same settings) prevents a galvanic connection (and thus any current) from flowing between the A and B electrodes; this seems important for electrode pairs placed on opposite sides of your body to prevent current through your heart.
The pulses have no DC component, so the actual wire polarity doesn’t really matter, but a foolish consistency definitely simplifies going back to re-measure things. Subsequent waveforms show the voltage with respect to the unmarked (outer) conductor.
Suppressing the DC bias prevents ionic migration between / under the electrode pads. The classic RC-equivalent output circuit uses a series capacitor, resulting in an asymmetric pulse waveform with zero net DC voltage:

There’s no DC path between the center and outer conductors, but in this day and age the circuitry could be a completely isolated bipolar FET driver:

With all that sorted out, I can make measurements!

Comments
4 responses to “Auvon TENS/EMS: Lead Identification”
The last time I looked inside one of those things was quite a while back, the circuitry then was pretty simple, a 555 driving a transistor switching a step-up transformer.
This generation definitely improves on the old waveforms, although it’s not at all obvious to me what (if any) effect fancy pulses have on the (claimed) therapeutic results.
[…] Auvon AS8016 TENS/EMS unit produces bipolar pulses with no net DC offset, so the UI controls the negative and positive […]
[…] scope screen shots use the same test setup as the pulse […]